Update 13/12/2011: EU patent on our key technology for minimal invasive pericardial access with the AttachLifter is granted.
Press release by TransMIT
The
"Standard" on Interventional Pericardiology Pericardioscopy and epi- and pericardial biopsy - a new window to the heart improving etiological diagnoses and permitting targeted intrapericardial therapy. Maisch B, Rupp H, Ristic A, Pankuweit S. Heart Fail Rev. 2013;18:317-28.  Subxiphoid approach with Tuohy needle  cleverfood.com |
Inflammatory
heart disease, i.e. carditis, remains an
ill-defined disorder caused by viral or
bacterial infection and autoimmune processes.
Often pericardial effusion ("fluid around the
heart") occurs. When pericardial effusion has
to be removed and drugs have to be instilled
into the pericardial space, the pericardium
must be punctured without injuring the
underlying heart muscle. Extensive
experience has been accumulated with the conventional
access to the pericardial sac using a blunt Tuohy
needle. This requires, however, a large pericardial
effusion which clearly separates the heart muscle from
the pericardium and thus reduces the risk of
puncturing the myocardium leading to life threatening
cardiac tamponade or haemopericardium (bleeding from
the punctured ventricle into the pericardial sac, the
distended pericardial sac prevents adequate filling of
the heart leading to severely depressed pump function,
shock and death). Many cardiologists
are fearful of using the conventional technique unless
severe pericardial effusion and thus also tamponade
(originating e.g. from pericardial inflammation or
cancer) is present, a situation in which the volume of
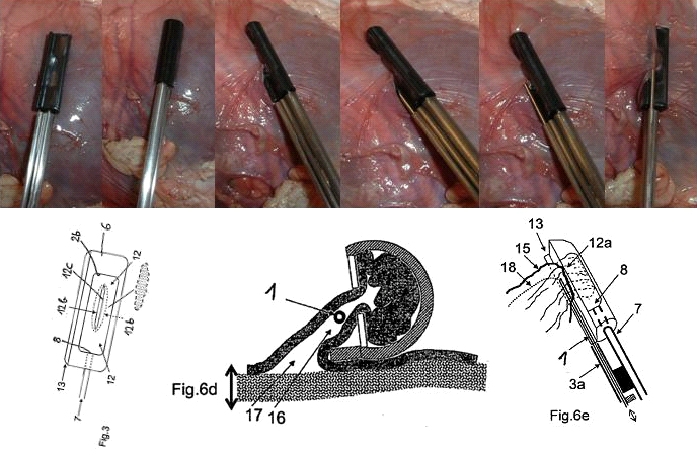
the effusion is at least 500 ml. The key technology is now available for accessing the pericardial space in a minimal invasive approach. The PeriAttacher provides a solution to the critical step of tissue puncturing by monitoring tissue attachment before the puncturing step. The AttachLifter permits also puncturing of thickened pericardium. No competing device available that works for thickened pericardium. Pioneering technology with prospects of future intrapericardial therapy interventions. It is timely to invest and strengthen this line of minimal invasive access to the pericardial sac (in-licencing opportunity). 
|
